
Successful Aging among Immigrant and Canadian-Born Older Adults: Findings from the Canadian Longitudinal Study on Aging (CLSA)

Abstract
:1. Introduction
1.1. Background
1.2. Conceptual Framework
1.3. Study Aims
- Do immigrants have (a) a greater prevalence and (b) higher age-sex adjusted odds of successful aging than their Canadian-born peers in the 2015–2018 wave of the Canadian Longitudinal Study on Aging (CLSA) comprehensive cohort?
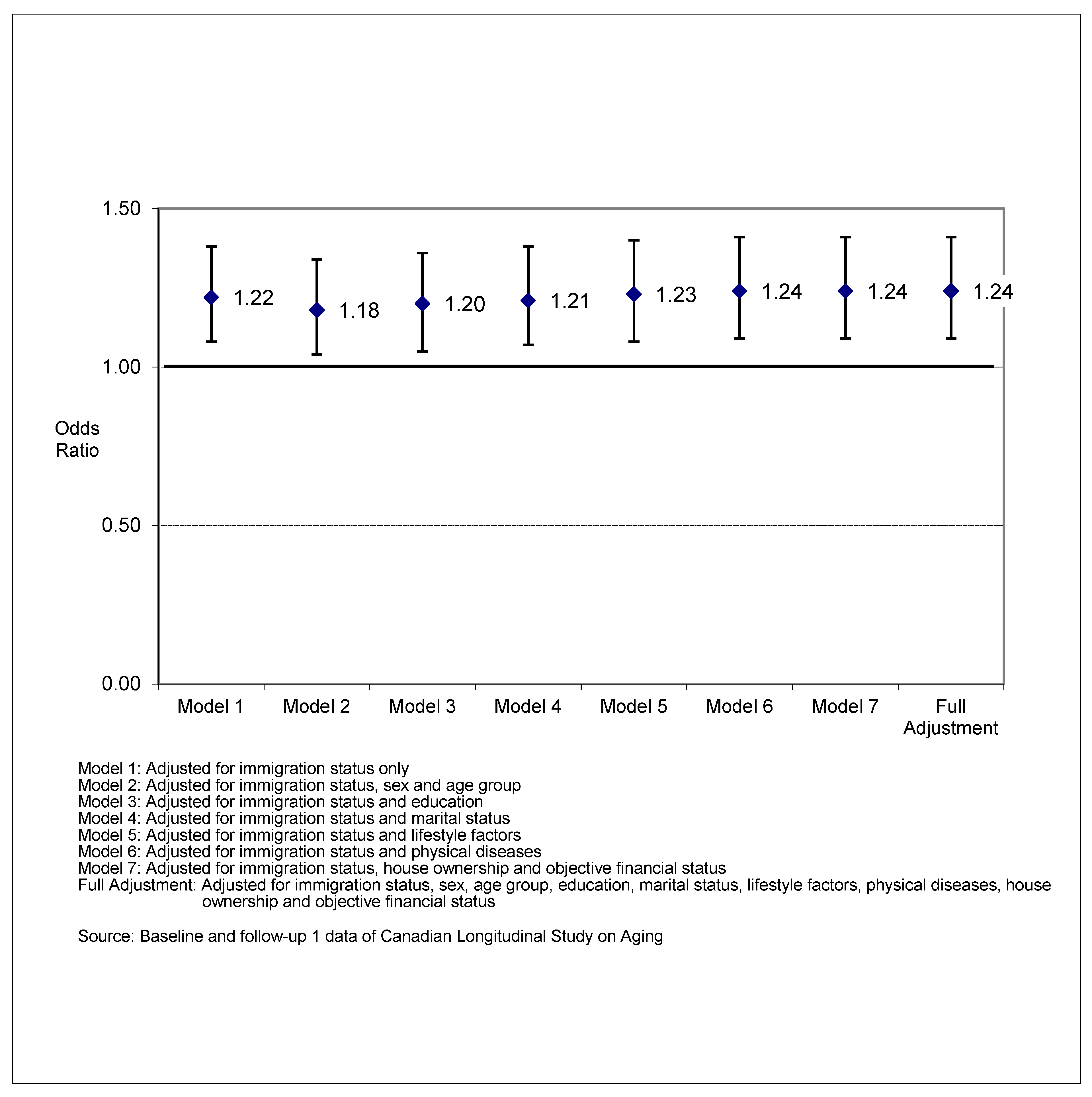
- What baseline factors, if any, attenuate the association between immigrant status and subsequent successful aging?
- Among immigrants, what baseline characteristics predict successful aging during the follow-up wave?
2. Materials and Methods
2.1. Study Population
2.2. Measures
2.2.1. Dependent Variables Assessed at Both Baseline and Time 2
2.2.2. Covariates
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Statistical Analysis
- Research Question 1a: Do immigrants have a greater prevalence of successful aging than their Canadian-born peers in the 2015–2018 wave of the Canadian Longitudinal Study on Aging (CLSA) comprehensive cohort?
- Research Question 1b: Do immigrants have higher age-sex adjusted odds of successful aging than their Canadian-born peers in the 2015–2018 wave of the Canadian Longitudinal Study on Aging (CLSA) comprehensive cohort?
- Research Question 2: What baseline factors, if any, attenuate the association between immigrant status and subsequent successful aging?
- Research Question 3: Among immigrants, what baseline characteristics predict successful aging during the follow-up wave?
3.3. Assessment of Model Fit
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Havighurst, R.J. Successful aging. Gerontologist 1961, 1, 8–13. [Google Scholar] [CrossRef]
- Pruchno, R.; Carr, D. Successful Aging 2.0: Resilience and Beyond. J. Gerontol. B Psychol. Sci. Soc. Sci. 2017, 72, 201–203. [Google Scholar] [CrossRef]
- Rowe, J.W.; Kahn, R.L. Successful aging 2.0: Conceptual expansions for the 21st century. J. Gerontol. B Psychol. Sci. Soc. Sci. 2015, 70, 593–596. [Google Scholar] [CrossRef] [Green Version]
- Meng, X.; D’Arcy, C. Successful aging in Canada: Prevalence and predictors from a population-based sample of older adults. Gerontology 2014, 60, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Tate, R.B.; Lah, L.; Cuddy, T.E. Definition of successful aging by elderly Canadian males: The Manitoba Follow-Up Study. Gerontologist 2003, 43, 735–744. [Google Scholar] [CrossRef] [Green Version]
- Goldhar, J.; Daub, S.; Dhalla, I.; Ellison, P.; Purbhoo, D.; Sinha, S.K. Integrated client care for frail older adults in the community: Preliminary report on a system-wide approach. Healthc. Q. 2014, 17, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Kuluski, K.; Gill, A.; Naganathan, G.; Upshur, R.; Jaakkimainen, R.L.; Wodchis, W.P. A qualitative descriptive study on the alignment of care goals between older persons with multi-morbidities, their family physicians and informal caregiver. BMC Fam. Pract. 2013, 14, 133–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greene, R.R.; Cohen, H.L.; Galambos, C.M.; Kropf, N.P. Foundations of Social Work Practice in the Field of Aging: A Competency-Based Approach; Port City Press: Baltimore, MD, USA, 2005. [Google Scholar]
- Moyle, W.; Parker, D.; Bramble, M. Care of Older Adults: A Strength-Based Approach; Cambridge University Press: Port Melbourne, Australia, 2014. [Google Scholar]
- About the CLSA Research Platform. Available online: https://www.clsa-elcv.ca/about-us/about-clsa-research-platform (accessed on 28 August 2022).
- Pruchno, R. Successful aging: Contentious past, productive future. Gerontologist 2015, 55, 1–4. [Google Scholar] [PubMed] [Green Version]
- Liang, J.; Luo, B. Toward a discourse shift in social gerontology: From successful aging to harmonious aging. J. Aging Stud. 2012, 26, 327–334. [Google Scholar] [CrossRef]
- Fernández-Ballesteros, R. The concept of successful aging and related terms. In The Cambridge Handbook of Successful Aging, 1st ed.; Fernández-Ballesteros, R., Benetos, A., Robine, J.M., Eds.; Cambridge University Press: Cambridge, UK, 2019; pp. 6–22. [Google Scholar]
- Cosco, T.D.; Prina, A.M.; Perales, J.; Stephan, B.C.M.; Brayne, C. Lay perspectives of successful ageing: A systematic review and meta-ethnography. BMJ Open 2013, 3, e002710. [Google Scholar] [CrossRef] [PubMed]
- Cosco, T.D.; Prina, A.M.; Perales, J.; Stephan, B.C.M.; Brayne, C. Operational definitions of successful aging: A systematic review. Int. Psychogeriatr. 2014, 26, 373–381. [Google Scholar] [CrossRef]
- Cosco, T.D.; Prina, A.M.; Perales, J.; Stephan, B.C.M.; Brayne, C. Whose “successful aging”? Lay- and researcher-driven conceptualizations of ageing well. Eur. J. Psychiat. 2014, 28, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Depp, C.A.; Jeste, D.V. Definitions and predictors of successful aging: A comprehensive review of larger quantitative studies. Am. J. Geriatr. Psychiatry 2006, 14, 6–20. [Google Scholar] [CrossRef]
- Bowling, A. Lay perceptions of successful aging: Findings from a national survey of middle aged and older adults in Britain. Eur. J. Ageing 2006, 3, 123–136. [Google Scholar] [CrossRef] [Green Version]
- Montross, L.P.; Depp, C.; Daly, J.; Reichstadt, J.; Golshan, S.; Moore, D.; Sitzer, D.; Jeste, D.V. Correlates of self-rated successful aging among community-dwelling older adults. Am. J. Geriatr. Psychiatry 2006, 14, 43–51. [Google Scholar] [CrossRef]
- Romo, R.D.; Wallhagen, M.I.; Yourman, L.; Yeung, C.C.; Eng, C.; Micco, G.; Pérez-Stable, E.J.; Smith, A.K. Perceptions of successful aging among diverse elders with late-life disability. Gerontologist 2012, 53, 939–949. [Google Scholar] [CrossRef] [Green Version]
- Chronic Conditions among Seniors Aged 65 and Older, Canadian Health Survey on Seniors. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310078801 (accessed on 28 August 2022).
- Canadian Survey on Disability Reports: A Demographic, Employment and Income Profile of Canadians with Disabilities Aged 15 Years and Over. 2017. Available online: https://www150.statcan.gc.ca/n1/pub/89-654-x/89-654-x2018002-eng.htm (accessed on 28 August 2022).
- Antón, J.I.; Braña, F.J.; Muñoz de Bustillo, R. An analysis of the cost of disability across Europe using the standard of living approach. SERIEs 2016, 7, 281–306. [Google Scholar] [CrossRef] [Green Version]
- Banks, L.M.; Kuper, H.; Polack, S. Poverty and disability in low- and middle-income countries: A systematic review. PLoS ONE 2017, 12, e0189996. [Google Scholar] [CrossRef] [Green Version]
- Young, Y.; Frick, K.D.; Phelan, E.A. Can successful aging and chronic illness coexist in the same individual? A multidimensional concept of successful aging. JAMDA 2009, 10, 87–92. [Google Scholar] [CrossRef]
- Focus on Geography Series, 2016 Census. Available online: https://www12.statcan.gc.ca/census-recensement/2016/as-sa/fogs-spg/Index-Eng.cfm (accessed on 28 August 2022).
- Notice—Supplementary Information for the 2021–2023 Immigration Levels Plan. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/news/notices/supplementary-immigration-levels-2021–2023.html (accessed on 28 August 2022).
- McDonald, J.T.; Kennedy, S. Insights into the “healthy immigrant effect”: Health Status and Health Service Use of Immigrants to Canada. Soc. Sci. Med. 2004, 59, 1613–1627. [Google Scholar] [CrossRef] [PubMed]
- The Healthy Immigrant Effect and Mortality Rates. Available online: https://www150.statcan.gc.ca/n1/en/pub/82-003-x/2011004/article/11588-eng.pdf?st=wI96mQh9 (accessed on 28 August 2022).
- Vang, Z.M.; Sigouin, J.; Flenon, A.; Gagnon, A. Are immigrants healthier than native-born Canadians? A systematic review of the healthy immigrant effect in Canada. Ethn. Health 2017, 22, 209–241. [Google Scholar] [CrossRef] [PubMed]
- Omariba, D.W.R. Immigration, ethnicity, and avoidable mortality in Canada, 1991–2006. Ethn. Health 2015, 20, 409–436. [Google Scholar] [CrossRef]
- Antecol, H.; Bedard, K. Immigrants and immigrant health. In Handbook of the Economics of International Migration; Chiswick, B.R., Miller, P.W., Eds.; Elsevier: Amsterdam, The Netherlands, 2015; Volume 1, pp. 271–314. [Google Scholar]
- Constant, A.F.; García-Muñoz, T.; Neuman, S.; Neuman, T. A “healthy immigrant effect” or a “sick immigrant effect”? Selection and policies matter. Eur. J. Health Econ. 2018, 19, 103–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, C.; Ng, E. Healthy immigrant effect by immigrant category in Canada. Health Rep. 2019, 60, 3–11. [Google Scholar]
- Liu, J.; Dong, X.Q.; Nguyen, D.; Lai, D.W.L. Family relationships and depressive symptoms among Chinese older immigrants in the United States. J. Gerontol. Ser. A 2017, 72 (Suppl. S1), S113–S118. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Xu, L.; Chi, I. Challenges and resilience related to aging in the United States among older Chinese immigrants. Aging Ment. Health 2018, 22, 1548–1555. [Google Scholar] [CrossRef]
- Wong, S.T.; Yoo, G.J.; Stewart, A.L. Examining the types of social support and the actual sources of support in Older Chinese and Korean immigrants. Int. J. Aging Hum. Dev. 2005, 61, 105–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, S.; Dupre, K.; Bosman, C. Moving to another country: Understanding the characteristics of the neighbourhood environment that influence the wellbeing of older Chinese immigrants. Geoforum 2022, 134, 13–21. [Google Scholar] [CrossRef]
- Khvorostianov, N.; Elias, N.; Nimrod, G. ‘Without it I am nothing’: The internet in the lives of older immigrants. New Media Soc. 2012, 14, 583–599. [Google Scholar] [CrossRef]
- George, U.; Thomson, M.S.; Chaze, F.; Guruge, S. Immigrant mental health, a public health issue: Looking back and moving forward. Int. J. Environ. Res. Public Health 2015, 12, 13624–13648. [Google Scholar] [CrossRef] [Green Version]
- Kwak, K. Age and gender variations in healthy immigrant effect: A population study of immigrant well-being in Canada. JIMI 2018, 19, 413–437. [Google Scholar] [CrossRef]
- Johnson, S.; Bacsu, J.; McIntosh, T.; Jeffery, B.; Novik, N. Competing challenges for immigrant seniors: Social isolation and the pandemic. HMF 2021, 34, 266–271. [Google Scholar] [CrossRef]
- Cha, N.H.; Seo, E.J.; Sok, S.R. Factors influencing the successful aging of older Korean adults. Contemp. Nurse 2021, 41, 78–87. [Google Scholar] [CrossRef]
- Salari, S. Invisible in aging research: Arab Americans, Middle Eastern immigrants, and Muslims in the United States. Gerontologist 2002, 42, 580–588. [Google Scholar] [CrossRef]
- Satariano, W.A. Epidemiology of Aging: An Ecological Approach; Jones & Bartlett Learning: Burlington, MA, USA, 2005. [Google Scholar]
- Smedley, B.D.; Syme, S.L. (Eds.) Promoting Health: Intervention Strategies from Social and Behavioral Research; National Academics Press: Washington, DC, USA, 2000. [Google Scholar]
- Wahl, H.W.; Iwarsson, S.; Oswald, F. Aging well and the environment: Toward an integrative model and research agenda for the future. Gerontologist 2012, 52, 306–316. [Google Scholar] [CrossRef]
- Katz, S.; Calasanti, T. Critical perspectives on successful aging: Does it “appeal more than it illuminates?”. Gerontologist 2015, 55, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Teater, B.; Chonody, J.M. How do older adults define successful aging? A scoping review. Int. J. Aging Hum. Dev. 2020, 91, 599–625. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Keyes, C.L.M. The mental health continuum: From languishing to flourishing in life. J. Health Soc. Behav. 2002, 43, 207–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Data Collection. Available online: https://www.clsa-elcv.ca/researchers/data-collection (accessed on 28 August 2022).
- Raina, P.S.; Wolfson, C.; Kirkland, S.A.; Griffith, L.E.; Oremus, M.; Patterson, C.; Tuokko, H.; Penning, M.; Balion, C.M.; Hogan, D.; et al. The Canadian Longitudinal Study on Aging (CLSA). Can. J. Aging CLSA Spec. Issue 2009, 28, 221–229. [Google Scholar] [CrossRef]
- Lin, P.S.; Hsieh, C.C.; Cheng, H.S.; Tseng, T.J.; Su, S.C. Association between physical fitness and successful aging in Taiwanese older adults. PLoS ONE 2016, 11, e0150389. [Google Scholar] [CrossRef] [PubMed]
- Hann, D.; Winter, K.; Jacobsen, P. Measurement of depressive symptoms in cancer patients. Evaluation of the Center for Epidemiological Studies Depression Scale (CES-D). J. Psychosom. Res. 1999, 46, 437–443. [Google Scholar] [CrossRef]
- Radloff, L.S. The CED-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Prins, A.; Bovin, M.J.; Smolenski, D.J.; Mark, B.P.; Kimerling, R.; Jenkins-Guarnieri, M.A.; Kaloupek, D.G.; Schnurr, P.P.; Kaiser, A.P.; Leyva, Y.E.; et al. The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5): Development and evaluation within a Veteran primary care sample. J. Gen. Intern. Med. 2016, 31, 1206–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Tong, H.; Lung, Y.; Lin, S.; Kobayashi, K.M.; Davison, K.M.; Agbeyaka, S.; Fuller-Thomson, E. Refugee status is associated with double the odds of psychological distress in mid-to-late life: Findings from the Canadian Longitudinal Study on Aging. Int. J. Soc. Psychiatry 2020, 67, 747–760. [Google Scholar] [CrossRef] [PubMed]
- Low-Income Measure (LIM) Thresholds by Income Source and Household Size. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1110023201 (accessed on 28 August 2022).
- Estebsari, F.; Dastoorpoor, M.; Khalifehkandi, Z.R.; Nouri, A.; Mostafaei, D.; Hosseini, M.; Esmaeili, R.; Aghababaeian, H. The concept of successful aging: A review article. Curr. Aging Sci. 2020, 13, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Martinson, M.; Berridge, C. Successful aging and its discontents: A systematic review of the social gerontology literature. Gerontologist 2015, 55, 58–69. [Google Scholar] [CrossRef] [Green Version]
- Sadarangani, T.R. Newly arrived early immigrants: A concept analysis of “aging out of place”. J. Transcult. Nurs. 2014, 26, 110–117. [Google Scholar] [CrossRef]
- Stewart, M.; Shizha, E.; Makwarimba, E.; Spitzer, D.; Khalema, E.N.; Nsaliwa, C.D. Challenges and barriers to services for immigrant seniors in Canada: You are among others but you feel alone. Int. J. Migr. Health Soc. Care 2011, 7, 16–32. [Google Scholar] [CrossRef]
- Canêdo, A.C.; Lopes, C.S.; Lourenço, R.A. Prevalence of and factors associated with successful aging in Brazilian older adults: Frailty in Brazilian older people Study (FIBRA RJ). Geriatr. Gerontol. Int. 2018, 18, 1280–1285. [Google Scholar] [CrossRef]
- Cosco, T.D.; Stephan, B.C.M.; Brayne, C.; Muniz, G.; MRC CFAS. Education and successful aging trajectories: A longitudinal population-based latent variable modelling analysis. Can. J. Aging 2017, 36, 427–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamid, T.A.; Momtaz, Y.A.; Ibrahim, R. Predictors and prevalence of successful aging among older Malaysians. Gerontology 2012, 58, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Ren, X.; Li, J.; Wu, K.; Wang, Y.; Chen, Q.; Li, N. Association between obesity status and successful aging among older people in China: Evidence from CHARLS. BMC Public Health 2020, 20, 767. [Google Scholar] [CrossRef] [PubMed]
- Singh-Manoux, A.; Sabia, S.; Bouillon, K.; Brunner, E.J.; Grodstein, F.; Elbaz, A.; Kivimaki, M. Association of body mass index and waist circumference with successful aging. Obesity 2014, 22, 1172–1178. [Google Scholar] [CrossRef] [Green Version]
- Dogra, S.; Stathokostas, L. Sedentary behavior and physical activity are independent predictors of successful aging in middle-aged and older adults. J. Aging Res. 2012, 2012, 190654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleg, J.L. Aerobic exercise in the elderly: A key to successful aging. Discov. Med. 2012, 13, 223–228. [Google Scholar]
- Sabia, S.; Singh-Manoux, A.; Hagger-Johnson, G.; Cambois, E.; Brunner, E.J.; Kivimaki, M. Influence of individual and combined healthy behaviours on successful aging. CMAJ 2012, 184, 1985–1992. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Byles, J.E.; Xu, X.; Zhang, M.; Wu, X.; Hall, J.J. Association between nighttime sleep and successful aging among older Chinese people. Sleep Med. 2016, 22, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Curcio, C.L.; Pineda, A.; Quintero, P.; Rojas, A.; Muñoz, S.; Gómez, F. Successful aging in Colombia: The role of disease. GGM 2018, 4, 2333721418804052. [Google Scholar] [CrossRef] [Green Version]
- Arias-Merino, E.D.; Mendoza-Ruvalcaba, N.M.; Arias-Merino, M.J.; Cueva-Contreras, J.; Arias, C.V. Prevalence of successful aging in the elderly in Western Mexico. Curr. Gerontol. Geriatr. Res. 2012, 2012, 460249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troutman, M.; Nies, M.A.; Small, S.; Bates, A. The development and testing of an instrument to measure successful aging. Res. Gerontol. Nurs. 2011, 4, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Cené, C.W.; Dilworth-Anderson, P.; Leng, I.; Garcia, L.; Benavente, V.; Rosal, M.; Vaughan, L.; Coker, L.H.; Corbie-Smith, G.; Kim, M.; et al. Correlates of successful aging in racial and ethnic minority women age 80 years and older: Findings from the Women’s Health Initiative. J. Gerontol. A. Biol. Sci. Med. Sci. 2016, 71 (Suppl. S1), S87–S99. [Google Scholar] [CrossRef] [PubMed]
- Kok, A.A.K.; Aartsen, M.J.; Deeg, D.J.H.; Huisman, M. Capturing the diversity of successful aging: An operational definition based on 16-year trajectories of functioning. Gerontologist 2017, 57, 240–251. [Google Scholar] [CrossRef] [Green Version]
- Gallardo-Peralta, L.P.; Muñoz, C.M.; Higuera, A.S. Health, social support, resilience and successful ageing among older Chilean adults. Int. Soc. Work 2022, 65, 283–299. [Google Scholar] [CrossRef]
- Social Isolation of Seniors: A Focus on New Immigrant and Refugee Seniors in Canada. Available online: https://www.canada.ca/en/employment-social-development/corporate/seniors/forum/social-isolation-immigrant-refugee.html (accessed on 28 August 2022).
- Highest Certificate, Diploma or Degree (15), Major Field of Study–Classification of Instructional Programs (CIP) 2016 (14), School Attendance (3), Age (13A) and Sex (3) for the Population Aged 15 Years and Over in Private Households of Canada, Provinces and Territories, Census Divisions and Census Subdivisions, 2016 Census—25% Sample Data. 2016 Census of Population. Statistics Canada Catalogue no. 98-400-X2016242. Ottawa. Available online: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/dt-td/Rp-eng.cfm?LANG=E&APATH=3&DETAIL=0&DIM=0&FL=A&FREE=0&GC=0&GID=0&GK=0&GRP=1&PID=110634&PRID=10&PTYPE=109445&S=0&SHOWALL=0&SUB=0&Temporal=2017&THEME=123&VID=0&VNAMEE=&VNAMEF= (accessed on 28 August 2022).


{kind=link}
| Variable | Definition |
|---|---|
| Limitations in Activity of Daily Living (ADL) | Based on yes/no response to five questions on (1) ability to dress and undress oneself without help; (2) ability to eat without help; (3) ability to walk without help; (4) ability to walk with some help from a person or with the use of a walker or crutches, etc.; (5) ability to get in and out of bed without any help or aids. Coded as “no” if answered “no” to all of the five questions. |
| Limitations in Instrumental Activity of Daily Living (IADL) | Based on yes/no response to eight questions on (1) ability to use the telephone without help; (2) ability to get to places out of walking distance without help; (3) ability to go shopping for groceries or clothes without help; (4) ability to prepare own meals without help; (5) ability to do housework without help; (6) ability to do housework with some help; (7) ability to take own medicine without help; (8) ability to handle own money without help. Coded as “no” if answered “no” to all of the eight questions. |
| Disabling pain or discomfort | Derived from responses to two questions that asked if respondents were usually free of pain or discomfort (yes/no) and the number of activities prevented by the pain or discomfort (none, a few, some, most). Coded as “no” if “free from pain or discomfort” and “none or a few activities prevented by the pain or discomfort.” |
| Mental disorders—Anxiety, Depression, Posttraumatic Stress Disorder (PTSD) | Derived from responses to three questions that were (1) based on yes/no response to a question that asked if respondents had ever been told by a doctor that they had an anxiety disorder such as a phobia, obsessive-compulsive disorder or a panic disorder; (2) based on the Centre for Epidemiological Studies Short Depression Scale (CES-D 10) score, coded as not having depression if the CES-D 10 score < 10 [56,57]; (3) coded as not having PTSD based on the Primary Care Posttraumatic Stress Disorder (PC-PTSD) score < 3 [58]. |
| Memory problems | Based on a yes/no question that asked if respondents had ever been told by a doctor that s/he had a memory problem. Coded as “no” if the respondents answered “no.” |
| Low mood—Felt depressed, felt happy, felt satisfied with life | Derived from responses to three questions that asked how often respondents felt depressed; felt happy; and felt satisfied with life [59] (all of the time (5–7 days), occasionally (3–5 days), some of the time (1–2 days), rarely or never (less than 1 day)). Coded as “no” if the respondents answered, “felt depressed rarely or never, or some of the time,” “felt happy occasionally or all of the time,” and “felt satisfied with life occasionally or all of the time.” |
| Lack of social support | Derived from responses to three questions that asked if respondents had (1) someone to give advice about a crisis; (2) someone who showed love and affection; (3) someone to confide in or talk to about oneself or one’s problems (none of the time, a little of the time, some of the time, most of the time, all of the time) [60]. Coded as “no” if the respondents answered “most of the time or all of the time” in all three questions. |
| Lack of self-rated wellness | Derived from responses to three questions that asked respondents to rate their (1) aging process; (2) perception of physical health; and (3) perception of mental health. Coded as “no” if the respondents answered “good to excellent” in all three questions. |
| Successful aging | Derived from responses to yes/no questions on (1) Limitations in ADL; (2) Limitations in IADL; (3) Disabling pain or discomfort; (4) Memory disorders; (5) Memory problems; (6) Low mood; (7) Lack of social support; (8) Lack of self-rated wellness. Coded as “yes” if the respondents answered “no” to all of these questions. |
| Household Size | Total | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Person | 2 Persons | 3 Persons | 4 Persons | 5 Persons | 6 Persons | 7 Persons | 8 Persons | 9 Persons | 10 Persons | |||
| Household Income | <$20,000 | 756 | 184 | 44 | 16 | 7 | 8 | 0 | 0 | 0 | 2 | 1017 |
| $20,000–$49,999 | 2134 | 2123 | 322 | 108 | 38 | 20 | 1 | 2 | 0 | 0 | 4748 | |
| $50,000–$99,999 | 1293 | 4525 | 676 | 238 | 76 | 30 | 8 | 4 | 2 | 0 | 6852 | |
| $100,000–$149,999 | 266 | 2032 | 403 | 195 | 36 | 12 | 3 | 0 | 3 | 0 | 2950 | |
| >$150,000 | 119 | 1329 | 356 | 171 | 45 | 10 | 6 | 0 | 0 | 0 | 2036 | |
| Don’t know | 254 | 241 | 40 | 14 | 5 | 3 | 4 | 1 | 0 | 0 | 562 | |
| Refused | 200 | 485 | 73 | 30 | 9 | 3 | 0 | 0 | 0 | 0 | 800 | |
| Total | 5022 | 10,919 | 1914 | 772 | 216 | 86 | 22 | 7 | 5 | 2 | 18,965 | |
| Legend | ||||||||||||
| Under poverty line income | ||||||||||||
| Marginal income | ||||||||||||
| Above poverty line income | ||||||||||||
| Not answered | ||||||||||||
| Variables | Successful Agers | Typical Agers | x2 (df), p-Value | % of Successful Agers |
|---|---|---|---|---|
| Immigrant Status | ||||
| Non-immigrant | 4443 (82%) | 1762 (78%) | 20.6 (1), p < 0.001 | 72% |
| Immigrant | 948 (18%) | 498 (22%) | 66% | |
| Sex | ||||
| Male | 2774 (52%) | 1161 (51%) | 0.005 (1), p = 0.946 | 71% |
| Female | 2617 (49%) | 1099 (49%) | 70% | |
| Age groups (years at baseline) | ||||
| 55–59 | 879 (16%) | 285 (13%) | 189.7 (5), p < 0.001 | 76% |
| 60–64 | 1630 (30%) | 449 (22%) | 77% | |
| 65–69 | 1232 (23%) | 476 (21%) | 72% | |
| 70–74 | 771 (14%) | 351 (16%) | 69% | |
| 75–79 | 613 (11%) | 405 (18%) | 60% | |
| 80+ | 266 (5%) | 244 (11%) | 52% | |
| Education | ||||
| <Secondary school graduation | 186 (4%) | 127 (6%) | 24.4 (2), p < 0.001 | 60% |
| Secondary school graduate and/or with some post-secondary education | 836 16%) | 390 (17%) | 68% | |
| Post-secondary degree/Diploma | 4369 (81%) | 1743 (77%) | 72% | |
| Mortgage | ||||
| Paying rent | 585 (11%) | 363 (16%) | 40.5 (2), p < 0.001 | 62% |
| Paying mortgage | 1164 (22%) | 478 (21%) | 71% | |
| Paid off mortgage | 3642 (68%) | 1419 (63%) | 72% | |
| Poverty line status | ||||
| Under poverty line income | 88 (2%) | 85 (4%) | 101.4 (3), p < 0.001 | 51% |
| Marginal income | 932 (17%) | 553 (25%) | 63% | |
| Above poverty line income | 4047 (75%) | 1461 (65%) | 74% | |
| No answer | 324 (6%) | 161 (7%) | 67% | |
| Marital status (at baseline) | ||||
| Single, never married or never lived with a partner | 219 (4%) | 137 (6%) | 68.0 (3), p < 0.001 | 62% |
| Married | 4273 (79%) | 1606 (71%) | 73% | |
| Widowed | 413 (8%) | 274 (12%) | 60% | |
| Divorced/Separated | 486 (9%) | 243 (11%) | 67% | |
| BMI | ||||
| Underweight/Normal weight | 1745 (32%) | 645 (29%) | 25.1 (2), p < 0.001 | 73% |
| Overweight | 2403 (45%) | 978 (43%) | 71% | |
| Obese | 1243 (23%) | 637 (28%) | 66% | |
| Smoking status | ||||
| Never smoked | 1810 (34%) | 708 (31%) | 10.4 (2), p < 0.01 | 72% |
| Former smoker | 3393 (63%) | 1442 (64%) | 70% | |
| Current smoker | 188 (4%) | 110 (5%) | 63% | |
| Sitting activity | ||||
| Never/Seldom | 75 (1%) | 39 (2%) | 1.21 (1), p = 0.271 | 66% |
| Sometimes/Often | 5316 (99%) | 2221 (98%) | 71% | |
| Walking | ||||
| Never/Seldom | 1302 (23%) | 639 (28%) | 14.3 (1), p < 0.001 | 67% |
| Sometimes/Often | 4089 (76%) | 1621 (72%) | 72% | |
| Light sports | ||||
| Never/Seldom | 4723 (88%) | 2023 (90%) | 5.54 (1), p < 0.02 | 70% |
| Sometimes/Often | 668 (12%) | 237 (11%) | 74% | |
| Moderate sports | ||||
| Never/Seldom | 4979 (92%) | 2144 (95%) | 15.6 (1), p < 0.001 | 70% |
| Sometimes/Often | 412 (8%) | 116 (5%) | 78% | |
| Strenuous sports | ||||
| Never/Seldom | 4092 (76%) | 1859 (82%) | 37.2 (1), p < 0.001 | 69% |
| Sometimes/Often | 1299 (24%) | 401 (18%) | 76% | |
| Muscle & endurance exercises | ||||
| Never/Seldom | 4224 (78%) | 1803 (80%) | 1.94 (1), p = 0.164 | 70% |
| Sometimes/Often | 1167 (22%) | 457 (20%) | 72% | |
| Sleep problem | ||||
| Never/Rarely/Some of the time | 4085 (76%) | 1589 (70%) | 24.8 (1), p < 0.001 | 72% |
| Occasional/All of the time | 1306 (24%) | 671 (30%) | 66% | |
| Diabetes | ||||
| No | 4602 (85%) | 1866 (83%) | 9.54 (1), p < 0.005 | 71% |
| Yes | 789 (15%) | 394 (17%) | 67% | |
| Heart disease | ||||
| No | 4848 (90%) | 1928 (85%) | 33.5 (1), p < 0.001 | 72% |
| Yes | 543 (10%) | 332 (15%) | 62% | |
| Hypertension | ||||
| No | 3414 (63%) | 1301 (58%) | 22.4 (1), p < 0.001 | 72% |
| Yes | 1977 (37%) | 959 (42%) | 67% | |
| Arthritis | ||||
| No | 4911 (91%) | 2034 (90%) | 2.29 (1), p = 0.131 | 71% |
| Yes | 480 (9%) | 226 (10%) | 68% | |
| Osteoporosis | ||||
| No | 4873 (90%) | 2009 (89%) | 3.95 (1), p < 0.05 | 71% |
| Yes | 518 (10%) | 251 (11%) | 67% |
| Variables | Immigrant Status Only | Immigrant Status + Age & Sex | Fully Adjusted |
|---|---|---|---|
| Non-immigrant (ref. immigrant) | 1.22 (1.08, 1.38) | 1.18 (1.04, 1.34) | 1.24 (1.09, 1.41) |
| Female (ref. male) | 1.04 (0.94, 1.15) | 1.17 (1.04, 1.31) | |
| Age groups (ref. 80+) | |||
| 55–59 | 2.76 (2.19, 3.48) | 2.16 (1.68, 2.79) | |
| 60–64 | 3.01 (2.42, 3.73) | 2.50 (1.98, 3.16) | |
| 65–69 | 2.51 (2.01, 3.14) | 2.20 (1.73, 2.79) | |
| 70–74 | 1.92 (1.52, 2.43) | 1.73 (1.35, 2.21) | |
| 75–79 | 1.45 (1.14, 1.85) | 1.36 (1.06, 1.74) | |
| Education (ref. < secondary school graduation) | |||
| Secondary school graduate and/or with some post-secondary education | 0.99 (0.76, 1.31) | ||
| Post-secondary degree/Diploma | 1.05 (0.81, 1.36) | ||
| Wealth Measure (ref. paying rent) | |||
| Paying mortgage | 1.04 (0.86, 1.25) | ||
| Paid off mortgage | 1.14 (0.97, 1.34) | ||
| Poverty Line Status (ref. under poverty line income) | |||
| Marginal income | 1.25 (0.90, 1.74) | ||
| Above poverty line income | 1.76 (1.27, 2.45) | ||
| No answer | 1.58 (1.08, 2.30) | ||
| Marital status (ref. single, never married or never lived with a partner) | |||
| Married | 1.42 (1.11, 1.84) | ||
| Widowed | 1.28 (0.93, 1.75) | ||
| Divorced/Separated | 1.26 (0.93, 1.69) | ||
| BMI (ref. obese) | |||
| Underweight/Normal weight | 1.24 (1.07, 1.44) | ||
| Overweight | 1.20 (1.05, 1.37) | ||
| Smoking status (ref. current smoker) | |||
| Never smoked | 1.46 (1.12, 1.89) | ||
| Former smoker | 1.37 (1.07, 1.77) | ||
| Sitting activities (ref. never/seldom) | 1.37 (0.94, 2.00) | ||
| Walking (ref. never/seldom) | 1.07 (0.95, 1.21) | ||
| Light sports (ref. never/seldom) | 1.17 (0.99, 1.39) | ||
| Moderate sports (ref. never/seldom) | 1.35 (1.09, 1.67) | ||
| Strenuous sport (ref. never/seldom) | 1.45 (1.27, 1.66) | ||
| Muscle or endurance exercises (ref. never/seldom) | 0.93 (0.81, 1.06) | ||
| Sleep problem (ref. occasionally/all of the time) | 1.29 (1.15, 1.44) | ||
| Diabetes (ref. with condition) | 1.14 (0.98, 1.31) | ||
| Heart disease (ref. with the condition) | 1.22 (1.04, 1.43) | ||
| Hypertension (ref. with the condition) | 1.03 (0.92, 1.15) | ||
| Arthritis (ref. with the condition) | 1.30 (1.08, 1.56) | ||
| Osteoporosis (ref. with the condition) | 1.15 (0.97, 1.37) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, M.; Pullenayegum, E.; Burnes, D.; Fuller-Thomson, E. Successful Aging among Immigrant and Canadian-Born Older Adults: Findings from the Canadian Longitudinal Study on Aging (CLSA). Int. J. Environ. Res. Public Health 2022, 19, 13199. https://doi.org/10.3390/ijerph192013199
Ho M, Pullenayegum E, Burnes D, Fuller-Thomson E. Successful Aging among Immigrant and Canadian-Born Older Adults: Findings from the Canadian Longitudinal Study on Aging (CLSA). International Journal of Environmental Research and Public Health. 2022; 19(20):13199. https://doi.org/10.3390/ijerph192013199
Chicago/Turabian StyleHo, Mabel, Eleanor Pullenayegum, David Burnes, and Esme Fuller-Thomson. 2022. "Successful Aging among Immigrant and Canadian-Born Older Adults: Findings from the Canadian Longitudinal Study on Aging (CLSA)" International Journal of Environmental Research and Public Health 19, no. 20: 13199. https://doi.org/10.3390/ijerph192013199